A clinical and methodological analysis of The Cut’s flawed coverage of Internal Family Systems

Summary
This report provides a clinical and methodological analysis of The Cut’s article on Internal Family Systems (IFS) therapy and the Castlewood Treatment Centre controversy. The article presents IFS and its founder, Richard Schwartz, Ph.D., as dangerous and pseudoscientific, a thesis that rests on both factual and methodological failures, compounded by clear patterns of journalistic bias and sensationalism across several key themes:
1. Factual conflation and misrepresentation
The article engages in a misleading conflation of two distinct figures, merging the identities and actions of Mark Schwartz, Sc.D., the former clinical co-director of Castlewood Treatment Centre who was sued for malpractice related to recovered memory implantation1, and Richard “Dick” C. Schwartz, Ph.D., the founder of the IFS model2. By attributing Mark Schwartz’s directive and discredited practices to IFS and its founder, the article fundamentally misrepresents the model itself. This conflation not only distorts the factual record but also exemplifies a recurring journalistic pattern through using proximity and association to construct guilt where none exists.
2. Sensationalism and scapegoating
Therapists and professional commentators have described The Cut’s article as a “clickbait hit piece,” likened to “yellow journalism” rather than objective reporting. It employs dramatic rhetoric, invoking parallels to cults, recovered memory scandals and past therapy panics3, effectively portraying IFS as a modern incarnation of these discredited practices. Such framing provokes moral outrage rather than informed understanding, prioritizing emotional reaction over accuracy and balance.
3. Selective testimony and narrative framing
The article presents survivor narratives, most notably Elizabeth’s case, almost exclusively through the lens of the accused father. This framing marginalizes the voice of Elizabeth (a pseudonym), who recovered memories of sexual abuse that she continues to stand by (with the support of her mother). Regardless of the ultimate legal findings or the veracity of her memories, Elizabeth was a patient subjected to documented malpractice at Castlewood. By sidelining her perspective, the reporting echoes broader societal patterns of silencing survivors and reinforces harmful power dynamics that risk retraumatizing victims, including readers with lived experience of abuse who may find such framing distressing or invalidating.
4. Pseudoscience narrative and evidence dismissal
The article dismisses IFS as “pseudoscientific” by contrasting it with more established, symptom-management models, without acknowledging the legitimacy of depth-oriented trauma therapies or the complexities of psychotherapy research. It also ignores emerging empirical support for IFS, including its previous SAMHSA recognition as an evidence-based modality4,5, and overlooks well-documented funding and publication biases that skew comparisons between psychotherapy and pharmaceutical studies6,7.
5. Ad hominem framing and character undermining
The article undermines Richard Schwartz’s credibility through insinuation rather than evidence, emphasizing personal details (e.g., spirituality) and associations over clinical substance. It extends this tactic by citing figures such as Bessel van der Kolk, Gabor Maté and Thomas Hübl to suggest that IFS’s legitimacy depends on “questionable” allies rather than its own merits. References to their past affiliations or credentials, coupled with mocking language such as “celebrity acolytes” and “flattering endorsements” portray IFS’s rise as a fleeting, celebrity-driven trend rather than a legitimate clinical approach. This reflects a broader tension between established academic gatekeepers and emerging experiential therapies that challenge traditional hierarchies in mental health8. Such portrayals help preserve professional orthodoxy by dismissing innovation as unserious, regardless of growing empirical support or demonstrated clinical value. This rhetorical approach diverts attention from the model’s substance and may also deter clinicians and advocates from openly supporting IFS.
6. Failure of clinical context and ethical reporting
Beyond factual and rhetorical issues, the article demonstrates a lack of clinical understanding. It conflates trauma-healing and symptom-management paradigms, applies inconsistent methodological standards, and fails to convey the principles of non-pathologizing, non-directive therapeutic work that define IFS. Ethically, it fails in its duty to report responsibly on sensitive mental health issues, prioritizing provocation over trauma-informed sensitivity.
Ultimately, The Cut’s article attempts to do too much and achieves none of its aims. If its goal was to critique IFS on scientific grounds, it fails methodologically. If it sought to investigate cult-like practices, it fails journalistically. If it aimed to model trauma-informed reporting, it fails ethically. What it does succeed in producing is sensationalized, emotionally charged content that amplifies fear and controversy, advancing the author’s visibility rather than contributing to informed public discourse. This outcome underscores the central ethical concern of this analysis: that complex, sensitive clinical subjects were reduced to provocative soundbites at the expense of accuracy, compassion and public trust.

Introduction
Before examining the article in detail, it’s important to note that while IFS can be a powerful therapeutic approach for many, it is not suitable for all individuals or clinical contexts. Additional clinical considerations arise when working with highly dissociative or acutely unstable clients9, 10. Furthermore, it may not be the treatment of choice for short-term interventions with hospitalized patients, for those lacking adequate follow-up and containment, or in situations where stabilization-focused therapies are more appropriate11. These considerations warrant careful professional oversight and continued study, yet they remain distinct from the article’s flawed and biased portrayal of IFS and its founder. The IFS Institute has acknowledged these challenges and is actively addressing them through enhanced training standards and ongoing research initiatives12,13. This will be discussed further in a later section.
Two unrelated Schwartzes: conflation as journalistic malpractice
The lynchpin of the article’s argument is its deliberate conflation of two distinct individuals, a rhetorical tactic that misleads readers and renders its central thesis invalid. By positioning the Castlewood clinic’s director and the IFS model’s founder in close narrative proximity, the article invites the reader to confuse them, thereby falsely attributing the clinic’s malpractice to the IFS model itself.
Mark Schwartz, Sc.D.: This individual was the Clinical Co-Director of the Castlewood Treatment Center. He holds a doctorate from Johns Hopkins University and was the subject of multiple malpractice lawsuits. These suits accuse him of using hypnosis and other suggestive techniques to implant false, often bizarre and disturbing memories in patients (later found to involve implausible accounts of abuse and ritualized harm). His specializations are listed as eating disorders, sexual trauma and intimacy disorders.
Richard “Dick” C. Schwartz, PhD: This individual is the founder of the Internal Family Systems (IFS) model. He holds a PhD in Marriage and Family Therapy from Purdue University and has held academic positions at the University of Illinois at Chicago and Northwestern University.
The article’s rhetorical strategy hinges on attributing the alleged harms associated with Mark Schwartz’s methods directly to Richard Schwartz’s IFS model. However, as clarified in a recent statement from the IFS Institute:
“Castlewood was operated by Mark Schwartz. The IFS model was created by Richard Schwartz. They are not related and have not been in contact for many years. Richard Schwartz served as a consultant and staff trainer at Castlewood. As a consultant, he was included in some patient sessions but never worked as a therapist for Castlewood clients. Richard Schwartz was never named in any of the lawsuits related to Castlewood.”
In a personal statement, Richard Schwartz added:
“I am deeply saddened by the confusion and pain caused by the story published by New York Magazine. I have compassion for anyone who has been affected by the events alleged. I am grateful to the hundreds of people in our community who have shared heartfelt public comments and testimonials in support of the IFS model.14”
The critical journalistic failure, therefore, is not the mention of Richard Schwartz in the context of Castlewood (since a professional association did exist) but the equation of Castlewood’s discredited methods with the IFS therapeutic model. As the next section will show, the practices for which Mark Schwartz was sued directly contravene the foundational principles of IFS, which explicitly rejects directive, suggestive or interpretive interventions.
The Castlewood controversy: a case study in anti-IFS practice
The article’s central claim that the harms at Castlewood are representative of IFS does not withstand clinical or methodological scrutiny. A review of the practices alleged at Castlewood versus the established principles of IFS reveals that Mark Schwartz’s methods were not “bad IFS”; they were non-IFS.
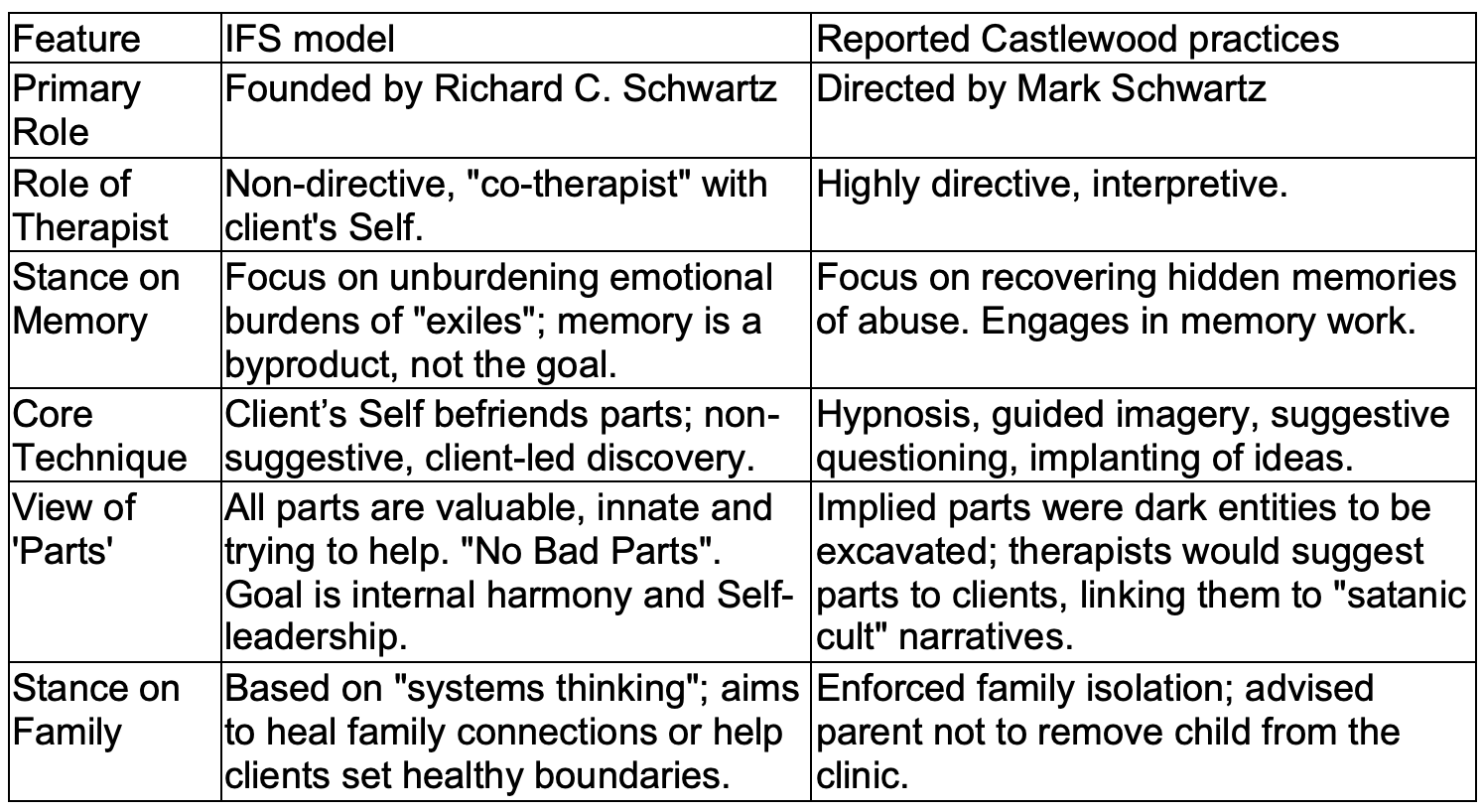
Reports and lawsuits concerning the Castlewood Treatment Center describe a disturbing revival of repressed memory therapy and “satanic panic” practices reminiscent of the 1990s15. These methods were highly directive rather than client-led, relying on hypnosis, guided imagery, dream interpretation and repeated suggestive cueing of traumatic memories. Patients were reportedly encouraged to recover memories of ritualistic abuse, such as belonging to “satanic cults” or enduring organized sexual exploitation, and were allegedly pressured into family isolation. In contrast, the IFS model is explicitly non-directive, non-suggestive and client-led. The therapist’s role is to help the client access their “Self” (the core, compassionate and calm centre of awareness) from which healing naturally unfolds. The therapist acts as a facilitator or “co-therapist,” never inventing, naming or assigning traits, parts or memories.
Where Castlewood pursued memory excavation, IFS focuses on memory reconsolidation, a neuroscience-informed process of revising emotional learning rather than recovering factual narratives. A recent meta-analysis supports this distinction, showing that non-directive instructions (reflective of IFS) carry a significantly lower risk of false memory implantation than guided imagery or pressure to respond (methods characteristic of Castlewood)16. The practices at Castlewood, therefore, directly violated the foundational principles of IFS. The Cut’s article mistakenly, and misleadingly, criticizes a non-directive model by invoking the well-documented harms of a highly directive one.
Comparative analysis: IFS model vs. Castlewood practice
The following table summarizes the fundamental, irreconcilable differences between the IFS model and the practices of Mark Schwartz’s clinic, which The Cut article conflates.
The article’s attempt to discredit Richard Schwartz extends well beyond its conflation with the Castlewood case, employing a consistent pattern of character assassination. It begins by citing an allegation that Schwartz was “careless” and once left “private medical documents on a park bench,” then selectively quotes from an interview, his social media posts, and his book No Bad Parts, while misrepresenting his spiritual orientation and benevolent collaborations with the Compassion Prison Project to portray him as incompetent, dangerous or delusional.
It should be acknowledged that the alleged act of removing confidential notes from a clinical setting and leaving them in a public space would, under U.S. law, constitute a breach of patient confidentiality and a violation of the Health Insurance Portability and Accountability Act (HIPAA). However, within the article, this reference functions rhetorically rather than evidentially, used to amplify a perception of recklessness while ignoring the clear separation between this isolated lapse and the documented malpractice of another individual, Mark Schwartz.
By strategically juxtaposing these details, the article blurs moral and professional boundaries, transferring culpability by association and reinforcing a false narrative that Richard Schwartz is a reckless practitioner and that the IFS model itself reflects that recklessness. This tactic is further advanced by invoking figures such as Bessel van der Kolk, Gabor Maté and Thomas Hübl to suggest that IFS’s legitimacy rests on “questionable” allies rather than its own scientific and clinical merits. References to their credentials and affiliations, coupled with mocking language such as “celebrity acolytes” and “flattering endorsements,” frame IFS’s rise as a fleeting, celebrity-driven trend rather than a legitimate therapeutic model.
This is particularly troubling given that the IFS model has been adopted by almost 15,000 practitioners worldwide (trained by the IFS Institute) and is increasingly integrated into trauma treatment settings. Many trauma survivors report meaningful recovery through IFS, supported by a growing (though still developing) body of empirical evidence13. If such individuals are discouraged from continuing treatment due to misleading or sensationalized reporting, the consequences could be severe. Undermining public trust in a therapeutic model that has demonstrably helped many clients risks not only reputational harm but also tangible psychological and emotional repercussions for those in care. In this sense, attempts to discredit a therapeutic modality and its founder may produce deeper and more far-reaching harm than the very misconduct the article purports to expose.
Misrepresentation of the client’s testimony
The article’s portrayal of the case in question relies on strategic omission and narrative framing. The story is told almost entirely from the perspective of the accused parent, whose pain and disbelief become the emotional centre of the piece. In contrast, the daughter (the actual patient) is rendered passive and voiceless. She is described through others’ interpretations rather than her own account, stripped of agency, perspective and complexity.
This framing leverages the deep emotional charge of parent–child estrangement to elicit automatic sympathy for the parent, positioning them as the unambiguous victim and the daughter as a misguided accuser. For readers who have experienced sexual abuse or been dismissed as unreliable, this dynamic risks retraumatization, reinforcing the societal pattern of disbelieving survivors.
The true tragedy, however, is not a daughter falsely accusing a parent, it is a family destroyed by clinical malpractice. The patient was treated in a facility where directive and suggestive techniques (methods long discredited for their potential to implant false memories) were reportedly used. Whether her recovered memories were accurate or not is now unknowable precisely because of those methods.
By focusing exclusively on the false memory narrative, the article centres the accused’s suffering while erasing the patient’s experience of harm. It commits a critical logical error: assuming that because some clients were harmed by unethical practices not related to the IFS model, the therapeutic model itself must be inherently dangerous. This conflation of a practitioner’s misconduct with the principles of an unrelated therapy represents both a methodological and ethical failure of journalism.
Finally, it is worth noting that experiences at Castlewood were not universally negative. Some former patients have described their treatment there as deeply beneficial or even “life-saving.” This complexity underscores the need for nuance: a single institution can both help and harm, depending on the integrity, competence and methods of individual clinicians.
Analyzing the “pseudoscience” claim
The article’s insinuation that IFS is a “pseudoscience” is factually incorrect and relies on a methodologically flawed understanding of how psychotherapy is evaluated.
Far from being an untested whim, IFS has a growing evidence base, a fact the article conveniently ignores.
SAMHSA NREPP Listing: In 2015, IFS was included in the U.S. government’s National Registry of Evidence-based Programs and Practices (NREPP), maintained by the Substance Abuse and Mental Health Services Administration (SAMHSA)17. The listing, based on an independent review process, rated IFS as “effective” for improving general functioning and well-being, and “promising” for phobia, panic and generalized anxiety disorders, depression, and self-concept18,19. The designation was supported by a 2013 randomized controlled trial (RCT) by Shadick et al., which found significant reductions in depression symptoms and physical pain among participants with rheumatoid arthritis20.
Trauma specific research: Although most existing studies on IFS and trauma are preliminary, they offer promising early evidence and form a foundation for ongoing large-scale RCTs.
- A 2021 pilot study evaluated IFS for adults with histories of childhood trauma. The study reported that “92% of participants no longer met criteria for PTSD at one-month follow-up” and concluded that IFS “shows strong potential as a trauma treatment deserving of further controlled study”21.
- A 2021 study examined the IFS concept of “Self-Leadership” (the capacity for compassion, calm and courage) and found it was uniquely associated with lower anxiety, depression, sleep disturbance and dissociation, as well as better relationship quality22.
- A 2024 study assessed the efficacy of IFS therapy for trauma-related symptoms. The study found significant reductions in PTSD symptoms and anxiety, supporting IFS as an effective trauma treatment approach warranting further research23.
- A 2024 study compared the effectiveness of IFS and Mindfulness-Based Cognitive Therapy (MBCT) in women with childhood trauma. Both therapies significantly decreased anxiety sensitivity and body dysphoria, suggesting IFS as a promising intervention for trauma-associated emotional and somatic symptoms24.
- A 2025 pilot study of an online hybrid group-and-individual IFS program for individuals with comorbid PTSD and substance use disorder demonstrated high acceptability and feasibility. The intervention produced clinically meaningful reductions in PTSD symptom severity and craving, indicating potential for integrated telehealth delivery of IFS to complex populations25.
Together, these studies illustrate a growing body of peer-reviewed evidence supporting IFS as a clinically promising, trauma-informed therapy, contradicting claims that it lacks empirical grounding26.
A methodological double standard (therapy vs. drug research)
The article’s critique of IFS reflects a methodological error common in popular and academic discourse: holding psychotherapeutic modalities to the evidentiary standards of pharmaceutical research. Such comparisons are conceptually invalid, as psychotherapy and pharmacotherapy differ fundamentally in mechanism, delivery and evaluative design. Large-scale RCTs, frequently idealized as the “gold standard” of evidence, are predominantly industry-funded and have been shown to overreport positive outcomes. By contrast, psychotherapy research faces intrinsic methodological constraints: it lacks equivalent financial support27, cannot employ double-blind designs, and must account for therapist allegiance effects28. To dismiss IFS as “pseudoscientific” for not conforming to pharmaceutical research standards, while disregarding the systemic biases underpinning those standards, constitutes a clear methodological and journalistic double standard.
The role and limitations of symptom-management models vs. IFS
The article’s critique reflects a limited clinical understanding, failing to distinguish between therapies designed for symptom management and those aimed at trauma resolution. In doing so, it attacks a depth model (IFS) for the dangers of depth, using as evidence a clinic that “went deep” in violation of ethical and methodological standards.
Contemporary, skills-based frameworks (often considered “gold-standard” treatments) are effective for stabilizing clients and managing symptoms. These structured, time-limited models emphasize cognitive restructuring, emotional regulation and coping strategies. Yet, as many clinicians note, they tend to prioritize symptom reduction over the deeper processing of traumatic experience. They offer essential tools for stabilization but may not reach the developmental and relational wounds underlying complex trauma.
By contrast, IFS represents a depth-oriented paradigm focused on healing at the source rather than solely managing surface symptoms. It is intentionally non-directive and non-pathologizing, helping clients engage compassionately with their internal “parts” and fostering integration through “Self-leadership”. The goal is not merely to control distress but to transform it by restoring internal harmony.
Criticizing IFS for not emphasizing symptom management reflects a category error. Both approaches serve vital but distinct therapeutic purposes, operate at different depths of intervention and address different phases of recovery29.
Acknowledging valid risks in a valid modality
The article, despite its flawed thesis, inadvertently highlights legitimate concerns within the mental health field. The harm it documents is real; however, it misattributes the cause. The genuine risks lie not so much in the IFS model itself, but in its misapplication by untrained or unethical practitioners.
While IFS can be a powerful therapeutic approach for many clients, it is not suitable for all individuals or clinical contexts, as discussed earlier. Another significant risk may stem from its recent popularity. This surge in interest has led to a proliferation of practitioners who may be inadequately trained or insufficiently supervised. For instance, the article notes that 45,000 mental health practitioners in the Psychology Today database list IFS as a treatment modality, whereas the IFS Institute has trained around 15,000. Where, then, have the remaining 30,000 practitioners been trained?
More broadly, the mental health field (including other modalities such as EMDR) faces structural issues that allow clinicians to complete non-accredited training programs without meaningful supervision or review of recorded sessions. Additionally, many graduate programs lack comprehensive trauma-informed curricula, leaving therapists vulnerable to oversimplified or misleading trainings on complex models like IFS, which they are not equipped to apply safely30,31.
This combination of unapproved training, insufficient prior clinical experience, lack of oversight, and failure to adhere to core IFS principles (rather than flaws within the model itself) constitutes the real danger. The well-documented harm at Castlewood, for example, did not occur because of IFS principles but due to their violation. Therapists (led by Mark Schwartz) imposed their own interpretations and asserted the therapist’s values rather than exploring the client’s values. Such directive, value-imposing practices directly contradict the fundamental IFS tenet of non-directiveness and client-led exploration. The problem, therefore, is not IFS, but the misapplication of IFS under its name.
As noted previously, another valid concern involves the use of IFS with clients experiencing high levels of dissociation, such as those with dissociative identity disorder (DID) or complex PTSD. Any depth-oriented therapy carries inherent destabilization risks if conducted without adequate grounding or when applied to individuals who are already highly dissociative. Competent IFS practice mitigates these risks through careful pacing, according to the client’s needs and limits. A skilled IFS therapist (trained by the IFS Institute and appropriately supervised) does not “go digging” for exiled parts (“exiles”) prematurely, as this can be destabilizing. Instead, trauma-informed application emphasizes first establishing a trusting relationship with the client’s protective parts (“managers” and “firefighters”). When applied correctly, IFS is generally not considered destabilizing; rather, it is the underlying trauma that contributes to dissociation, whereas poorly paced or inadequately trained therapy may overwhelm a client’s protective system.
In summary, the risks associated with IFS arise primarily from systemic issues in clinician training and from the model’s popularity outpacing its responsible dissemination, not from flaws within the theoretical framework itself. With proper training, supervision and trauma-informed pacing, IFS remains a valuable and safe modality for many individuals in clinical practice. That said, it is important to acknowledge that IFS, like any therapeutic approach (including CBT or DBT) may not be effective or suitable for every client, even when applied correctly.
Conclusion
The Cut’s article fails to serve the public good. It exploits a family tragedy, relies on a fundamental and disqualifying factual conflation of two different professionals, and misapplies methodological standards to paint a promising model as “pseudoscience”.
The article correctly identifies a harm (the malpractice at Castlewood) but completely misdiagnoses the pathogen. It attributes the harm to IFS, when the evidence clearly shows the harm was caused by the violation of IFS principles, namely the use of directive, suggestive and discredited recovered memory techniques. The real, valid concerns about IFS lie not so much in its model, which is evidence-based and non-pathologizing, but in its implementation. The true risk, as with any potent therapy, is destabilization by practitioners who are inadequately trained, poorly supervised, and who (like the therapists at Castlewood) violate the model’s most sacred, non-directive principles.
References
1. https://www.courthousenews.com/bizarre-claim-against-eating-disorder-clinic/
2. https://en.wikipedia.org/wiki/Richard_C._Schwartz
3. https://www.tandfonline.com/doi/full/10.1080/10538710802584601
4. https://foundationifs.org/news-articles/79-ifs-an-evidence-based-practice
5. https://foundationifs.org/research/empirical-evidence
7. https://pmc.ncbi.nlm.nih.gov/articles/PMC8951352/
8. https://pubmed.ncbi.nlm.nih.gov/40874484/
9. https://link.springer.com/article/10.1007/s44202-025-00339-2
11. https://www.tandfonline.com/doi/full/10.1080/10926771.2021.2013375
13. https://ifs-institute.com/resources/research
14. https://ifs-institute.com/news-events/news/response-new-york-magazine-article
15. https://cornerstone.lib.mnsu.edu/cgi/viewcontent.cgi?article=2328&context=etds
16. https://pubmed.ncbi.nlm.nih.gov/37113566/
17. https://foundationifs.org/news-articles/79-ifs-an-evidence-based-practice
19. https://ifs-association.com/wp-content/uploads/2013/12/IFS-Evidence-Based.pdf
20. https://pubmed.ncbi.nlm.nih.gov/23950186/
21. https://www.tandfonline.com/doi/full/10.1080/10926771.2021.2013375
22. https://www.tandfonline.com/doi/pdf/10.1080/01926187.2020.1865218
23. https://psycnet.apa.org/fulltext/2024-98110-001.html
25.https://www.frontiersin.org/journals/psychiatry/articles/10.3389/fpsyt.2025.1544435/full
29. https://pmc.ncbi.nlm.nih.gov/articles/PMC10845104
Excellent critique. Thank you
Wow, the conflation of Mark and Richard Schwartz really stood out. This systematic breakdown of journalistic failure is crucial. How can we collectively foster better media literacy to counteract such deliberate misrepresentation? Your analytical rigor here is truly commendable.